
Dutch cancer care: strong foundation, clear opportunities for improvement
New OECD/EU report shows where the Netherlands is doing well and where improvement is needed
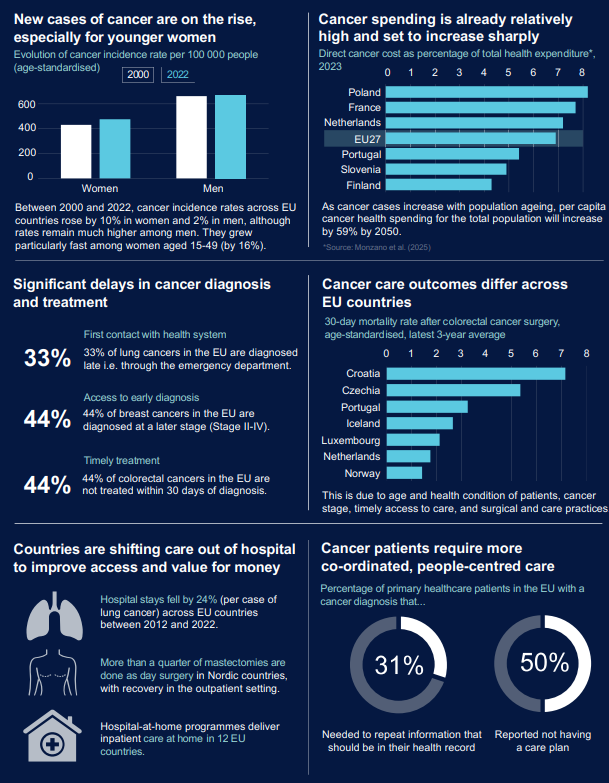
The report points to several urgent developments. For example, cancer among young women in Europe is increasing relatively quickly. Between 2000 and 2022, the number of cancer diagnoses (incidence) in EU countries rose by 10 percent among women and by 2 percent among men. The strongest growth was seen among women aged 15 to 49, where incidence increased by 16 percent. Although the total number of new cancer diagnoses among men is still higher, the picture is clearly shifting in younger age groups. This means that more women are confronted with years of treatment and follow-up at a young age, with a major impact on quality of life, work, and financial security, and with long-term pressure on healthcare systems. At the same time, the report identifies three priorities to create more value:
- Faster access to the right care through clear referral pathways and time standards;
- More care outside the hospital where possible;
- More attention to person-centred support, including palliative, psychosocial, and financial care, with good coordination and follow-up.
In the Netherlands, these developments also align with what we see in the data. IKNL previously showed that young women are 1.5 times more likely to develop cancer than young men. This means that a large group of people is already confronted at a young age with treatment, follow-up, and the consequences for work, family life, and quality of life. Against this background, the question is not only how we continue to deliver good cancer care, but above all how we organise it in such a way that it remains sustainable in the long term and meaningful for patients.
In this context, the OECD and the European Commission published their international comparison on high-value cancer care. The Netherlands performs strongly on several points, but the report also shows where improvement is needed. These are choices that determine whether care is available on time, whether patients receive the right treatment, and whether the organisation of care matches what people need. By measuring indicators for high-quality care per country, the report offers points for improvement to make cancer care more effective.
What is meant by ‘high-value cancer care’?
By high-value cancer care, the authors mean care that delivers as much health gain and quality of life as possible, with as little unnecessary burden as possible for patients and the healthcare system. It is based on three interrelated pillars:
- Accessible and timely care: rapid access to diagnostics and treatment, so that cancer is not detected unnecessarily late.
- Appropriate, evidence-based care: treatments that demonstrably help, and the prevention of overdiagnosis and overtreatment.
- Person-centred care: good alignment and coordination, with attention to quality of life and support during and after treatment.
This approach is necessary now that the number of people with cancer continues to rise and pressure on staff and budgets is increasing. Countries that steer explicitly in this direction achieve better outcomes at lower societal costs.
Strong starting position of the Netherlands
In the European comparative picture, the Netherlands stands out positively on a number of points. For example, the Netherlands is among the leaders in participation in colorectal cancer screening. This is above the European target value and is associated with a relatively high proportion of diagnoses at an early stage. Early detection increases the chance of less invasive treatment and better survival.
This effect is also visible in the outcomes. On 4 February—World Cancer Day—IKNL showed that the number of people with metastatic colorectal cancer in the Netherlands is showing a downward trend. This development is closely linked to the structural impact of colorectal cancer screening. It shows that investing in screening leads to fewer patients with advanced disease and fewer intensive treatments.
For cervical cancer, the Netherlands is also among the countries where a large proportion of cases is detected at an early stage. This is related to the organisation of and participation in the screening programme (including self-sampling), although unfortunately we are seeing a downward trend here as well. Research in 2025 also showed that young women in the Netherlands diagnosed with cervical cancer were often not vaccinated.
In addition, the Dutch cautious policy regarding PSA testing for prostate cancer fits within the broader movement towards appropriate care. Avoiding routine screening helps to limit overdiagnosis and unnecessary treatment and aligns with the aim of providing appropriate care with real health gains.
Where are we doing less well?
The report also shows that Dutch cancer care is vulnerable at a number of crucial points.
Participation in breast and cervical cancer screening has clearly declined since the COVID-19 period. Less screening increases the risk of later detection, more intensive treatments, and poorer outcomes. This also comes at the expense of the value of care.
A second concern is the large difference between planned care and emergency care in colorectal cancer. In the Netherlands, the risk of dying within 30 days after an emergency operation is much higher than after a planned operation. This makes it clear how important timely recognition and well-organised diagnostics are.
In prostate cancer as well, risks of overdiagnosis and overtreatment remain. International comparisons show large differences in how often prostate cancer in older men is detected at an early stage. This points to varying screening practices and the lack of uniform guidelines. For the Netherlands, this means that overdiagnosis can lead to substantial costs and unnecessary treatments, with an impact on quality of life, without proportional health gains.
The report further shows that in the Netherlands, gains can be made through better care coordination and more person-centred care. This includes more consistent use of care plans and better alignment between healthcare providers in the different phases of the disease process.
The role of data and cancer registries
A recurring theme in the report is the importance of good, comparable, and timely data to be able to steer policy towards value. Without insight into where delays occur, where over- or undertreatment takes place, and where outcomes differ, improvement remains largely guesswork.
Gijs Geleijnse, who on behalf of IKNL worked closely with the OECD on the development of the report, says:
If we want to seriously work towards high-value cancer care, we need to know where we stand and where we can improve. Cancer and quality registries are indispensable for this. International comparisons based on these registries show where patients are identified too late, where treatment practices differ, and where outcomes are improving or lagging behind. Without that data, you cannot develop targeted policy. Then ‘high-value cancer care’ remains an abstract concept instead of a concrete steering instrument.
According to Geleijnse, the international comparisons show that investing in good registries and data linkages is a prerequisite for learning and improving. It is the basis for measuring, comparing, and improving the quality, efficiency, and patient-centredness of cancer care.
Call to policymakers
The message of the report is relevant for Dutch policy on sustainable, accessible, high-quality cancer care. The greatest gains lie in organising care faster, smarter, and in a more person-centred way. This requires:
- Renewed commitment to screening and early detection, with attention to groups that are currently less well reached;
- Strengthening rapid diagnostic pathways to prevent emergency presentations;
- Continued focus on appropriate care: less overdiagnosis and overtreatment, more appropriate care;
- Investments in data availability for care and research, in order to be able to steer purposefully on quality and value.
The Netherlands has a strong starting position. At the same time, the report shows that standing still is not an option. In a time of growing demand for care and limited resources, steering towards high-value cancer care is not a luxury, but a necessity.
More information
For more information about this study, please contact Jolanda Sinha. See also the presentation by EU Commissioner Oliver Várhelyi during the launch of the report.